
July 2026 · The Evidence Era of Medicaid Prior Authorization
Medicaid PA Is Moving From Decision-Making to Decision Proof
Across June’s developments the expectation shifted from understanding policy to producing operational proof — that decisions were timely, clinically reviewed, properly noticed, and defensible.
June did not produce one sweeping Medicaid PA rule. It produced convergence — across reporting, automation oversight, notice adequacy, electronic PA readiness, state reform, and appeal defensibility — on a single operational message: prior authorization is entering the era of evidence.
Why This Matters Now
Live reporting, live state effective dates, formal federal recommendations, and a zero-for-100 denial audit mean organizations that wait for final rules will be building evidence controls after the oversight environment has already moved.
Operational Intelligence Signal
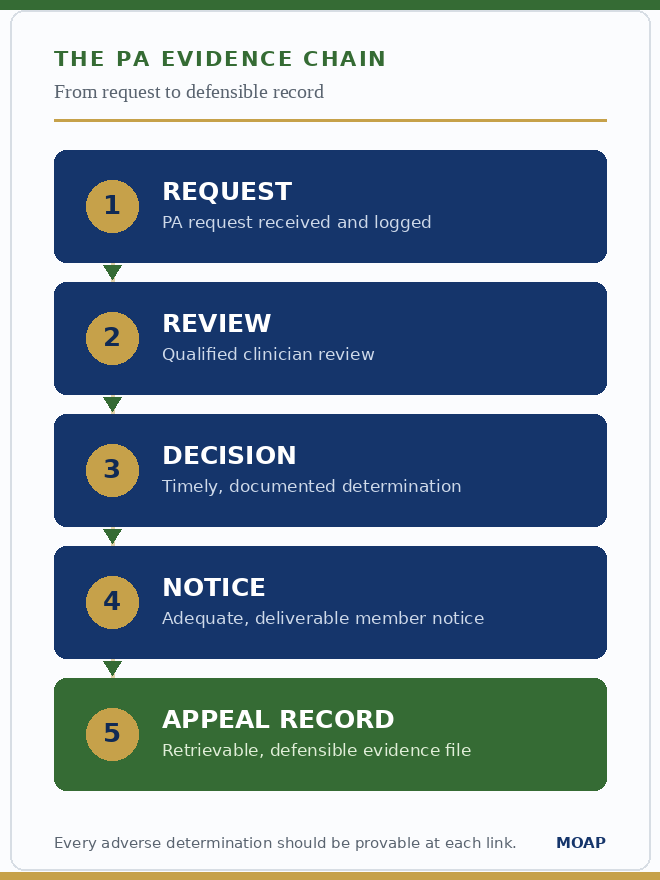
June’s dominant operational capability is defensible authorization and adverse-determination evidence. Every major signal — MCPAR data, automation-review records, notice adequacy, cross-plan authorization history, and appeal documentation — points to one requirement: proof. Organizations are no longer judged only on whether they make PA and appeal decisions, but on whether they can prove those decisions were timely, human-reviewed, properly noticed, and defensible. The burden is shifting from policy compliance to evidence readiness.
Executive Summary
Key Takeaways
- Transparency is becoming operational surveillance. MCPAR plan-level reporting makes PA denial rates, overturn rates, and decision times visible and comparable — plans need internal dashboards that mirror what CMS and states will see.
- Automation governance is becoming a documentation requirement. Human review, model testing, validation, bias evaluation, and oversight logs must be producible; automation use without an evidence file is becoming a governance exposure.
- The denial notice is now an auditable control. Notice content, delivery, address accuracy, record-access language, and appeal-rights language matter operationally — appeals risk begins before the appeal is filed.
- State reform is redesigning the burden itself. Massachusetts eliminated PA for broad categories while requiring continuity and 90-day cross-plan honoring.
- The operating model is becoming evidence-driven. The challenge is producing dated, traceable proof that decisions are timely, reviewed, noticed, reported, and transferable.
A Note From Jessica

Jessica TurnerFounder, MOAP
June wasn’t about one headline rule. The operational center of gravity moved toward defensibility — leaders are being asked to prove more. This month’s developments suggest the questions worth asking inside your own organization are:
- Can you prove the decision was timely?
- Can you prove a qualified human reviewed the denial?
- Can you prove the member’s notice was adequate and delivered?
- Can you prove your reported data match what your systems did?
- Can you prove an authorization can follow the member?
The risk isn’t that organizations don’t understand the policy direction. It’s that their workflows, data pipelines, templates, and records can’t yet support the proof now being expected.
The next operational advantage is evidence readiness.
Jessica
This Month
What Changed This Month
MACPAC Automation Recommendations Formalized
The June report formally recommends that adverse determinations not be made by automation alone, that plans disclose automation testing and oversight, and that similar expectations extend to FFS programs.
Commission RecommendationOIG: Zero of 100 Denials Compliant
An OIG audit of a Medicaid behavioral-health plan found none of 100 sampled denials fully met requirements — wrong addresses, unclear notices, missing record-access rights. Notice adequacy is now audit exposure.
Industry DataMCPAR Plan-Level PA Reporting Begins
June MCPAR submissions require plan-level PA volumes, approval and denial rates, appeal-overturn rates, and decision times — making PA performance comparable and visible.
Reporting RequirementMassachusetts Subtract-PA Model
Massachusetts eliminated PA for broad service categories (eff. June 5) while requiring 24-hour urgent responses, continuity for stable chronic conditions, and 90-day honoring of authorizations after plan switches.
State ActivityDrug PA Enters Final-Rule Phase
CMS-0062-P moved into its final-rule phase, keeping a proposed October 1, 2027 compliance date and a 24-hour outpatient-drug decision clock in play for pharmacy utilization management.
Proposed RuleIntelligence Brief
Inside OIG’s Medicaid Denial Audit: “Zero for 100”
What Happened
An HHS OIG audit of a Medicaid behavioral-health plan found that none of 100 sampled denied requests met all requirements — notices reached incorrect addresses, used unclear language, and omitted the enrollee’s right to request denial records free of charge. It is the first behavioral-health entry in OIG’s denial series.
Why It Matters
It reframes the denial notice from a clerical byproduct into an auditable control. Paired with MACPAC’s now-formal human-review recommendations, the bar is no longer a timely decision — it is a defensible, documented, properly communicated one.
Operational Risk
Missing notice copies, delivery proof, record-access language, and qualified-reviewer sign-offs surface in audit, appeal, or state review — and the notice step is usually unowned until a complaint exposes it.
Questions Leaders Should Be Asking
Could you pull ten recent denials and prove each notice met every requirement — and who owns the denial-to-notice-to-appeal handoff end to end?
“The decision is no longer enough. Medicaid organizations must be able to prove how the decision was made.”
Intelligence Question of the Month
Can we defend our PA and appeal performance externally with the same confidence we report it internally — producing proof of human review, notice adequacy, automation oversight, and timeliness on demand?
Operational Implications
Payer and Provider Perspectives
- Prioritize PA data integrity, denial-to-appeal linkage, and decision-time timestamps.
- Maintain qualified-human-review logs and an automation-disclosure file — including FFS.
- Audit notice-template adequacy: content, address, delivery, record-access language.
- Monitor vendor timeliness and keep corrective-action evidence.
- Build cross-plan authorization-history workflows so authorizations can travel.
The readiness issue cuts across UM, appeals, compliance, analytics, and IT.
- Strengthen criteria-aligned first submissions.
- Preserve denial notices and request full denial records when appropriate.
- Track plan timeliness and cite automation and notice deficiencies in appeals.
- Use emerging public metrics to support escalation.
- Give heightened attention to BH, pediatrics, specialty drugs, and chronic-condition services.
Provider engagement helps shape practical, workable policy.
At a Glance
Executive Risk Radar
Readiness Pressure
Monthly Readiness Index
Readiness pressure reflects how prepared organizations should be to respond — distinct from risk severity.
By the Numbers
Numbers That Matter
National Intelligence
State Spotlight
Key Changes · DOI Regulations (effective June 5, 2026)
Operational Question: If a new member arrived tomorrow with an active authorization from another plan, could your system honor it for 90 days — or would it make them start over?
Why This State Matters Nationally
Massachusetts represents a different reform model — subtract PA where possible, preserve continuity where needed, and require public PA-rule visibility. It moves beyond faster PA into redesigning the authorization burden itself, and previews the authorization-portability requirement arriving federally through the 2027 Payer-to-Payer API.
Operational Lessons
- Reconfigure UM rules engines to stop requiring PA for mandated categories.
- Stand up continuous chronic-condition authorization logic.
- Build 90-day cross-plan honoring with reliable authorization-history lookup.
- Re-baseline UM and appeals forecasts as volume redistributes.
Forward Look
Operational Outlook
MCPAR data-quality questions, CMS dashboard status, and OIG denial-audit attention remain active.
Automation-disclosure readiness and notice adequacy are likely to surface in state oversight, appeals, and vendor reviews.
Defensible PA evidence, human-review documentation, and interoperability readiness become executive differentiators.
Watchlist
Top 5 Items to Watch This Month
- CMS response to MACPAC automation recommendations. Watch for guidance or FFS rulemaking that converts the human-review principle into binding requirements.
- CMS-0062-P final-rule signals. Track the timeline toward the proposed October 1, 2027 compliance date and the 24-hour drug-PA decision clock.
- MCPAR data-quality feedback or FAQs. Reconcile plan-level volumes, overturn rates, and decision times against operations as the first cycle is reviewed.
- CMS appeals & grievance dashboard confirmation. Confirm go-live and scope; assume appeals timeliness and overturn outcomes become oversight intelligence.
- Additional OIG Medicaid MCO denial audits. Expect the denial-compliance series to widen — run a notice-adequacy self-audit now.
MOAP Readiness Spotlight
This month’s OIG finding makes the denial file an auditable control. A defensible file should hold, per adverse determination: the medical-necessity rationale and denial reason, the qualified-clinician review and sign-off, the timeliness log, the notice copy with proof of delivery and address accuracy, the record-access and appeal-rights language, and automation-oversight evidence — held to the same standard across delegated UM vendors.
Why This Matters
A denial you cannot evidence is exposure waiting for an audit, appeal, or state review. The operational issue is rarely policy knowledge — it is fragmented workflows and unowned handoffs that leave the file incomplete until someone asks for it.
Readiness Question
Could your team produce, within a day, a complete evidence file for any denial issued last quarter — notice copy, delivery proof, record-access language, and reviewer sign-off?
Building clarity, consistency, and confidence—together.
Join the Conversation
Follow Jessica Turner & Medicaid Operations Advisory Partners on LinkedIn for:
For the Record
Sources Referenced
- MCPAR — Managed Care Program Annual Report plan-level PA metrics (first cycle, June 2026)
- MACPAC June 2026 Report to Congress — Automation in Medicaid Prior Authorization recommendations
- HHS OIG — Behavioral-health managed-care denial-compliance audit
- Massachusetts DOI Regulations — Subtract-PA model with continuity protections (eff. June 5, 2026)
- CMS-0062-P — Interoperability Standards & Prior Authorization for Drugs (final-rule phase)
Operational and regulatory-monitoring insight only. Verify dates, audit findings, and comment deadlines against primary sources (CMS, the Federal Register, regulations.gov, MACPAC, HHS OIG) before relying on them.